

Background:
Hodgkin's lymphoma (HL) is the model of curative care with radiation therapy, combination chemotherapy, staging approaches, peripheral blood stem cell transplantation, and immunotherapy. However, the value of the novel anti cancer drugs has been recently analyzed and questioned in view of the results in the real improvement of overall survival (OS).
Material and methods:
All consecutive patients seeking medical care after 1986 in our institution as a result of HL and followed for at least 3 months were entered in the study. A diagnosis of HL was based on the histological study of a pathology specimen, mainly a lymph node; the same pathologist analyzed all the specimens and defined the histological subtype. Clinical stage was defined according to the Ann Arbor classification. Bone marrow biopsies were done only in patients with clinical stages III or IV. Computed tomography (CT) scans were done in all cases, prior to starting the treatment. Fluorodeoxyglucose positron emission tomography (FDG-PET) scans were performed since 2002. Between 1986 and 1997, patients were treated with MOPP, and after 1997 with ABVD as frontline therapy. For stages I and II, four cycles of chemotherapy were delivered and a computerized tomography (CT) scan was performed; if lymph node enlargement were present at this point in time, four additional cycles were given, whereas two additional cycles were given if the CT scan was negative. For stages III and IV, the CT scans were performed at the end of six cycles and two or four more cycles. Mediastinal radiotherapy was delivered only to persons with a positive FDG-PET scan at the end of the treatment. Patients showing activity after these treatments were considered as refractory and treated with four courses of ICE (ifosfamide, carboplatin and etoposide). Autologous or allogeneic peripheral blood hematopoietic stem cell transplants (HSCT) were given to refractory patients after achieving a complete remission (CR): High-dose melphalan (200mg/m2) was employed in autologous transplants, whereas cyclophosphamide, fludarabine and busulfan were employed in allogeneic transplants, all of them from HLA-identical siblings. After the completion of the treatment, patients were every two months for one year and every four months later on. No FDG-PET scans were done during the follow up, unless clinically indicated.
Results:
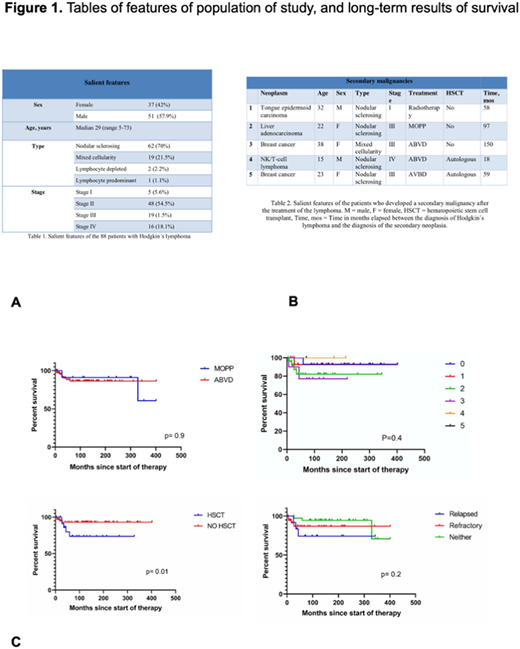
Among 91 patients with HL identified between 1986 and 2020, 88 were followed three months or more and were included in the analysis. There were 37 females and 51 males. The median age was 29years (range5-73years). There were 62 patients with nodular sclerosing HL (70%), 19 mixed cellularity (HL), 2 lymphocyte depleted HL, and one lymphocyte predominant HL; in 4 cases the histologic variant could not be defined. According to Ann Arbor classification, 5 patients were found in stage I, 48 in stage II, 19 in stage III and 16 in stage IV. Ten patients presented with a mediastinal mass larger than 10 cm. in the chest X-ray film. Three cases presented with relapsed disease. Patients have been followed for a median of 114 months (range4-402). 44 patients are alive, 10 have died and 34 were lost to follow-up. Median OS for all the patients has not been reached, being above 402 months, the OS at 310 months is 88% and at 402 months 77%. Median OS has not been reached and is above 94, 109, 90 and 98 months for stages I, II, III and IV, respectively (p=0.2). The 310-month OS was 83% for patients treated with MOPP and 88% for those treated with ABVD (HR:0.76, 95% CI 0.2-2.8; p=0.6).Sixteen patients (18%) were refractory to the treatment and 9 (10%) relapsed; they were treated with ICE followed by HSCT (autologous 15 patients and allogeneic 10 patients). Patients who underwent auto-HSCT had a median survival of 329.1 months and an OS of 92.3%, whereas those given allo-HSCT had a median survival of 59.3 months and an OS of 45.7% (HR0.2, 95%CI 0.04-1.3, p=0.057). The OS of patients given or not HSCT was 73.5% and 92.9% at 266 and 404 months, respectively (HR4.09, 95%CI 1.0-16.6, p=0.01). The OS was similar. The causes of death were breast carcinoma in 2 cases, liver carcinoma in one and uncontrolled lymphoma activity in the remaining.
Conclusion:
HL may be less aggressive in Mexican population than in Caucasians. Combined chemotherapy renders acceptable results, irrespective of clinical stage.
No relevant conflicts of interest to declare.

This feature is available to Subscribers Only
Sign In or Create an Account Close Modal